HOP: Why "Forklift Operator Error" Is Where the Investigation Fails
Human error is never the root cause—it's the starting point your investigation should never have stopped at.
HOP: Why "Forklift Operator Error" Is Where the Investigation Fails
A forklift strikes a pedestrian in the warehouse. The operator was texting. The incident report says "root cause: operator distraction, failure to follow safe operating procedures." Case closed. Training scheduled. Discipline issued.
And nothing changes.
Because "operator error" isn't a root cause—it's the moment your investigation gave up. Human and Organizational Performance (HOP) principles exist precisely because most safety investigations stop at the person and never touch the system that set them up to fail.
The Subangle: Why "Human Error" Root Causes Guarantee Repeat Incidents
Here's the actual scenario: the operator was texting because the warehouse uses a digital pick system that requires confirmation at every stop. Drivers are measured on picks per hour. There's no designated safe zone to check the device. The pedestrian walkway isn't painted—it was, but the striping wore off eight months ago and repainting got bumped for budget. The forklift has no proximity alarm because "we've never had an incident before."
The investigation found "operator distraction." It didn't find:
- A performance metric that penalizes stopping to check a device safely
- A facility design with no engineered separation between forklifts and pedestrians
- A maintenance backlog where safety infrastructure gets deferred
- A fleet without basic engineering controls despite known pedestrian traffic
So you retrain the operator. You discipline them. Maybe you fire them. And six months later, a different operator in the exact same system hits someone else.
The Five HOP Principles (and the One Everyone Ignores)
Todd Conklin's HOP framework has five principles. Most safety programs reference them. Few actually apply them. Here's the one that breaks most investigations:
Principle 1: Error is normal. Humans make mistakes. Designing a system that depends on perfect human performance is designing a system that will eventually fail. The question isn't "why did this person screw up?" The question is "why did our system allow this mistake to cause harm?"
When you write "human error" as your root cause, you're saying the system was fine—the human was the problem. HOP flips it: the human's behavior is normal. The system that made that behavior dangerous is the problem.
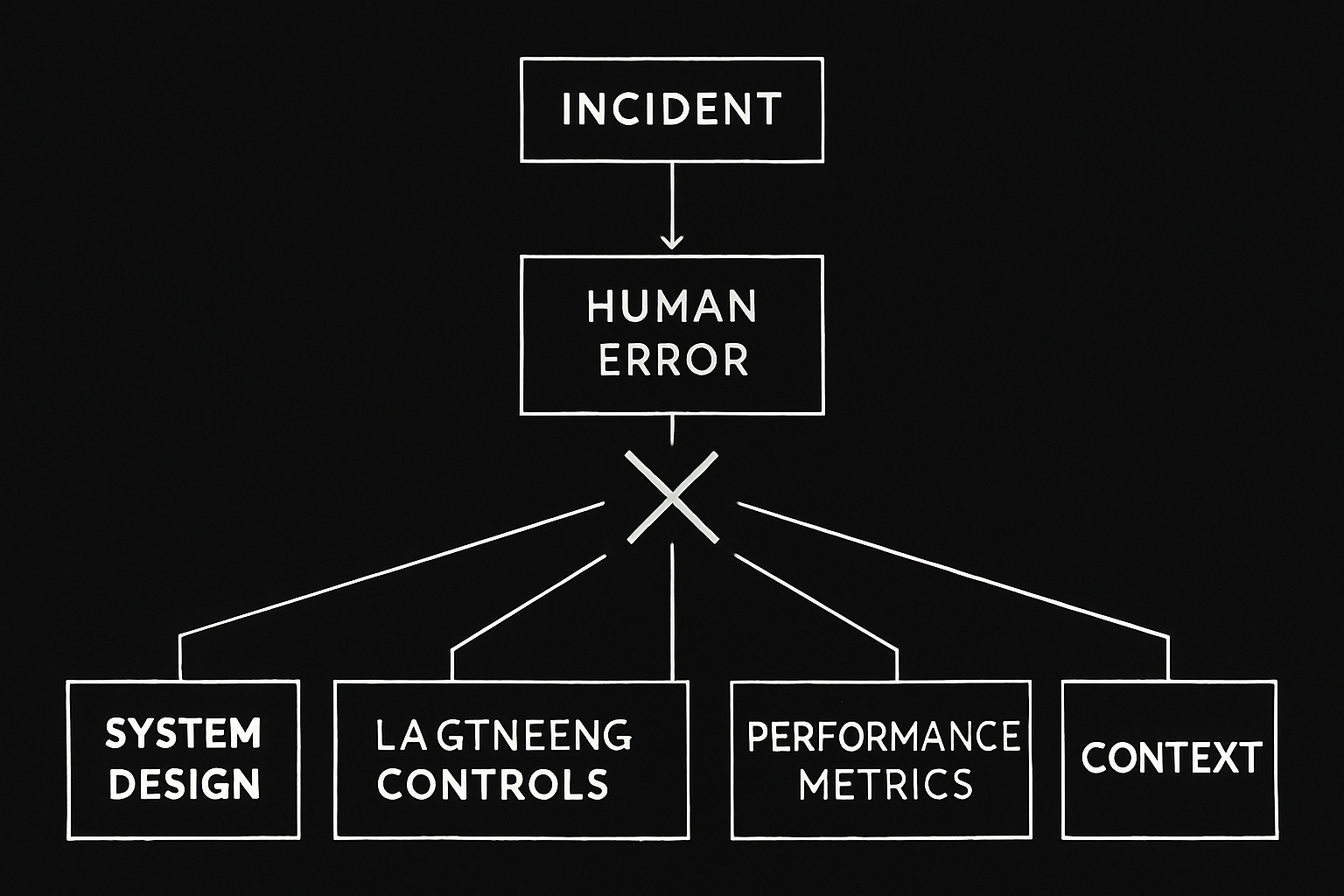
Here's what that investigation looks like under HOP:
- Error: Operator was distracted by device while driving.
- Context: Device is required for job task. Productivity is measured by speed. No safe zone exists to stop and check device. Distraction is not an anomaly—it's baked into the workflow.
- System failure: Performance metrics conflict with safe behavior. Engineering controls (proximity alarms, pedestrian barriers) are absent. Maintenance systems allowed safety infrastructure (striping) to degrade without replacement.
- Latent conditions: Budget prioritization defers safety spend. Fleet procurement standards don't include pedestrian detection technology. No formal Management of Change review when the pick system went digital and changed operator task demand.
Now you have something to fix. And it's not the operator.
Why Blame Fixes Nothing (and Makes Everything Worse)
Most companies treat incident investigations as fault-finding missions. Someone screwed up. Find them. Punish them. Send a message.
Here's what actually happens: near-miss reporting drops. People stop telling you about close calls because they've seen what happens to the last person who got "investigated." Your leading indicators—the only data that predicts where your next recordable is coming from—disappear. You're flying blind, and you did it to yourself.
HOP Principle 2: Blame fixes nothing. Punishing the person who touched it last doesn't change the system. It just teaches everyone else not to be the last person to touch it when something goes wrong.
The companies that stay stuck at Stage 2 on the Bradley Curve (Dependent safety culture—"I follow the rules when someone's watching") are the ones still running blame-based investigations. You can't supervise your way to an Interdependent culture. You have to build a system where people trust that telling you about problems won't get them fired.
What an Actual HOP Investigation Looks Like
Start with the error. Don't stop there.
Ask: What about the work environment made this behavior make sense to the person doing it? Not "why did they violate the rule?" but "what made violating the rule the logical choice in that moment?"
In the forklift case:
- Checking the device while moving saved 30 seconds per pick.
- Stopping safely to check the device would have dropped the operator below their productivity target.
- Pedestrians in the aisle was normal—there was no defined walkway and no physical barrier.
- No alarm warned the operator a person was in the blind spot.
The operator made a rational decision within a system that rewarded speed and provided no engineered safeguards. That's not "operator error." That's a system designed to eventually hurt someone.
FAQ: Human and Organizational Performance
What does HOP stand for in safety?
HOP stands for Human and Organizational Performance. It's a framework for understanding that human error is a symptom of system design failures, not a root cause. HOP principles focus on learning from incidents, eliminating blame, and redesigning systems to tolerate normal human variability.
Why is "human error" not a root cause?
Because it doesn't explain why the error occurred or how to prevent it. Saying "human error" is like saying "the car crashed because the driver lost control." It's technically true and completely useless. HOP pushes you to ask: what conditions made the error likely? What system failures allowed the error to cause harm?
How do HOP principles reduce incidents?
By shifting investigations from blame to learning. When people trust that reporting problems won't get them punished, near-miss reporting increases. That gives you leading indicator data to fix hazards before they become injuries. HOP also drives you toward engineering controls and system redesigns instead of relying on procedure compliance and supervision.
What's the connection between HOP and the Bradley Curve?
HOP principles are what move a company from Stage 2 (Dependent—safety by supervision) to Stage 4 (Interdependent—team-based safety culture). You can't mandate accountability. You build it by creating systems where people trust that speaking up about problems is safe and productive. That's HOP in practice.
If You're Still Writing "Human Error" as Root Cause, We Should Talk
Most safety programs plateau because the investigation process stops too early. You find the person. You retrain them. The same incident happens again with someone else.
If your incident investigations aren't surfacing system failures and latent conditions—if they're still stopping at "operator didn't follow procedure"—your program is stuck. And your TRIR reflects it.
We don't run investigations for clients, but we do handle the entire administrative load—OSHA 300 logs, training records, ISNetworld updates, program documentation—so in-house EHS managers actually have time to do root cause work that matters. If the admin burden is eating the time you should be spending on this, let's talk. Schedule a call here.
AW
Aaron West
Founder, EHS, Inc. — 18+ years in EHS compliance and contractor safety
Aaron West has spent over 18 years helping contractors and businesses navigate OSHA compliance, ISNetworld® certification, and workplace safety management. He founded EHS, Inc. to make enterprise-level EHS accessible to companies of all sizes — serving contractors and businesses nationwide — without long-term contracts or enterprise overhead.
Ready to simplify your EHS compliance?
Our team handles the complexity so you can focus on running your business. No long-term contracts, no learning curve.
Talk to EHSRelated Articles
Multi-Entity Risk Transfer Strategies for Reducing EMR Exposure
When one subsidiary's bad year tanks the parent company's EMR, you need risk transfer architecture—not more training reminders.
How to Dispute Medical-Only Claims Reclassified as Lost Time
One misclassified medical-only claim as lost time can inflate your EMR for three years and cost you tens of thousands in premiums.
How the Three-Year EMR Lookback Follows Your Company Through Every Bid
One incident in 2023 is still killing your bids in 2026. Here's what the EMR lookback actually costs you and what you can do about it.
Medium & Enterprise
Safety Culture System
Framework to achieve zero incidents
Get Free System →
Small Businesses
50+ Safety Topics
Stop hitting paywalls
Get Free Topics →
All Companies
Audio Safety Topics
54 topics in English & Spanish
Get Free Audio →